CLINICAL VIGNETTES
CASE 1
A 42-year-old man presents with a two-month history of fevers, night sweats, and unintentional weight loss. Physical examination reveals generalized lymphadenopathy and mild hepatosplenomegaly. Laboratory studies show mild anemia, thrombocytopenia, elevated C-reactive protein, and hypoalbuminemia. Autoimmune testing is negative. Imaging demonstrates multiple enlarged lymph nodes in the mediastinum and retroperitoneum.
Misdiagnosis
The patient was initially diagnosed with lymphoma and treated with rituximab. After two cycles with no improvement, he was referred for further evaluation.
Excisional Biopsy
A biopsy of a retroperitoneal lymph node was performed, revealing features consistent with idiopathic multicentric Castleman disease (iMCD).
Learn about grading follicular atresia and view examples.
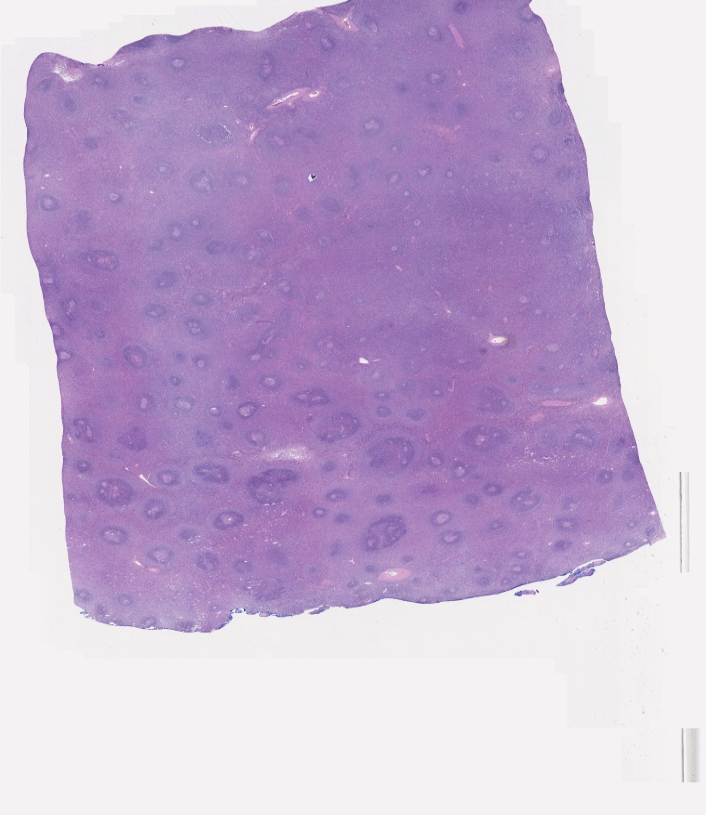
Click the image to view the low-power biopsy and see follicular structures
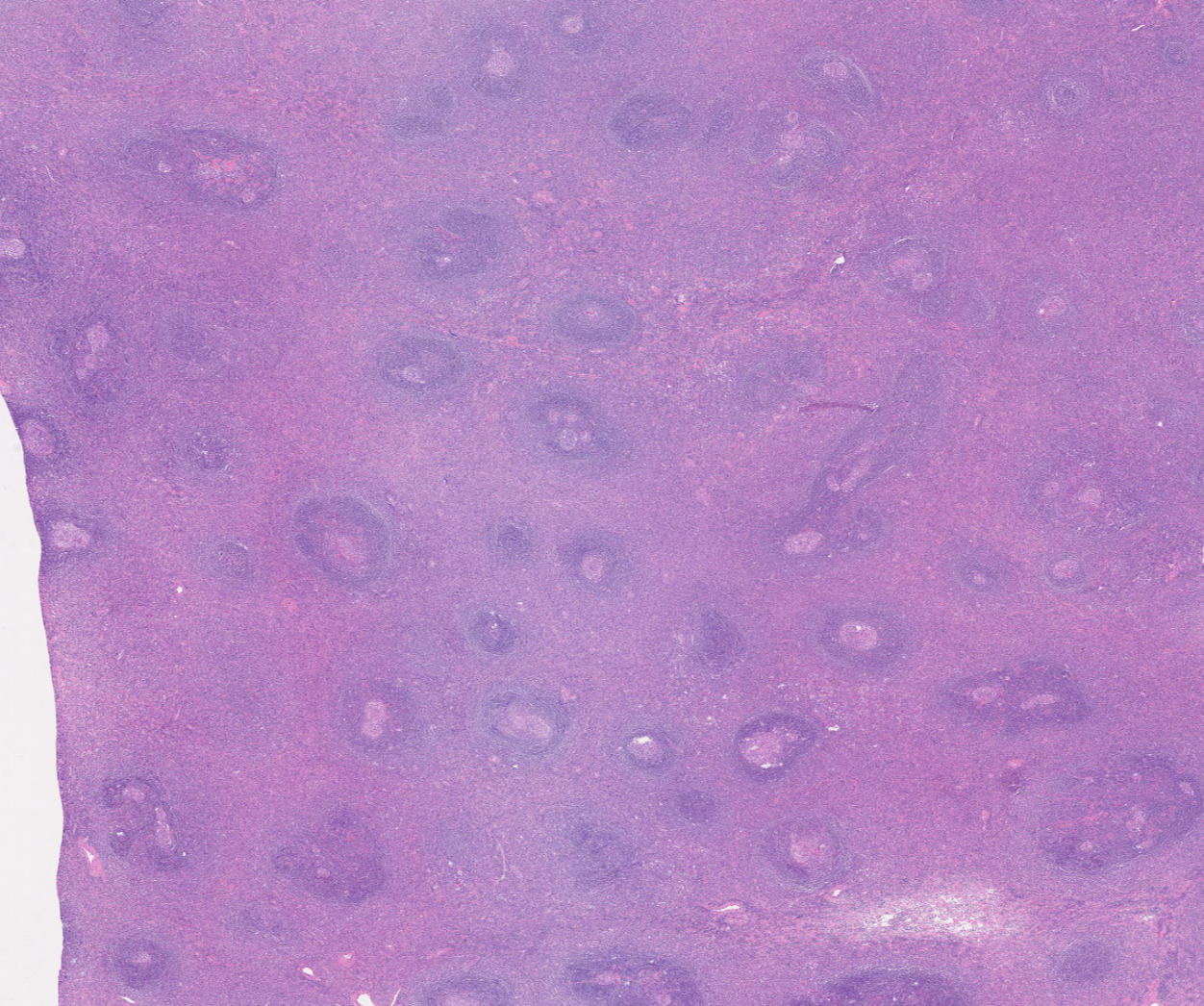
Medium-power magnification demonstrated clearly atrophic germinal centers
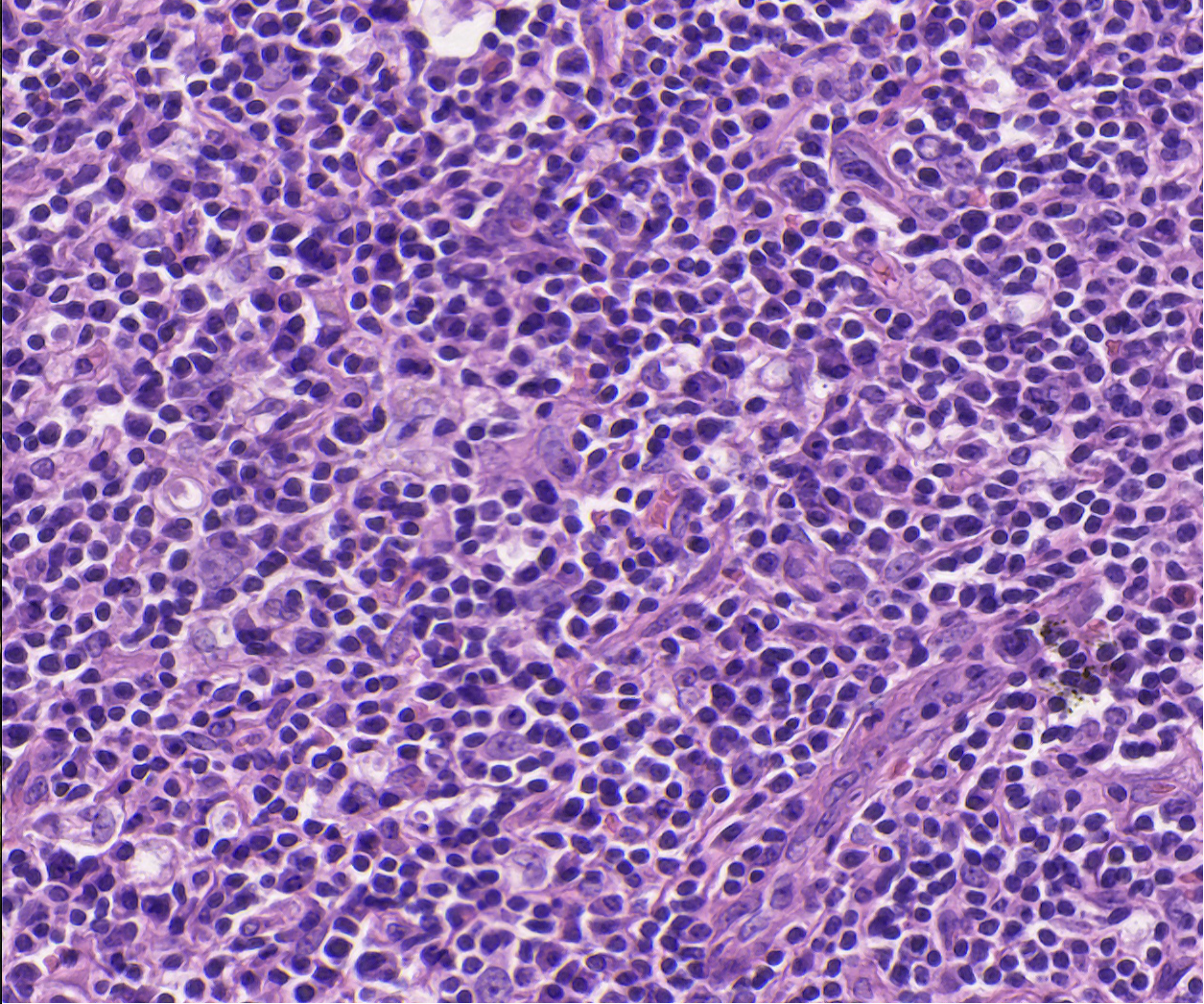
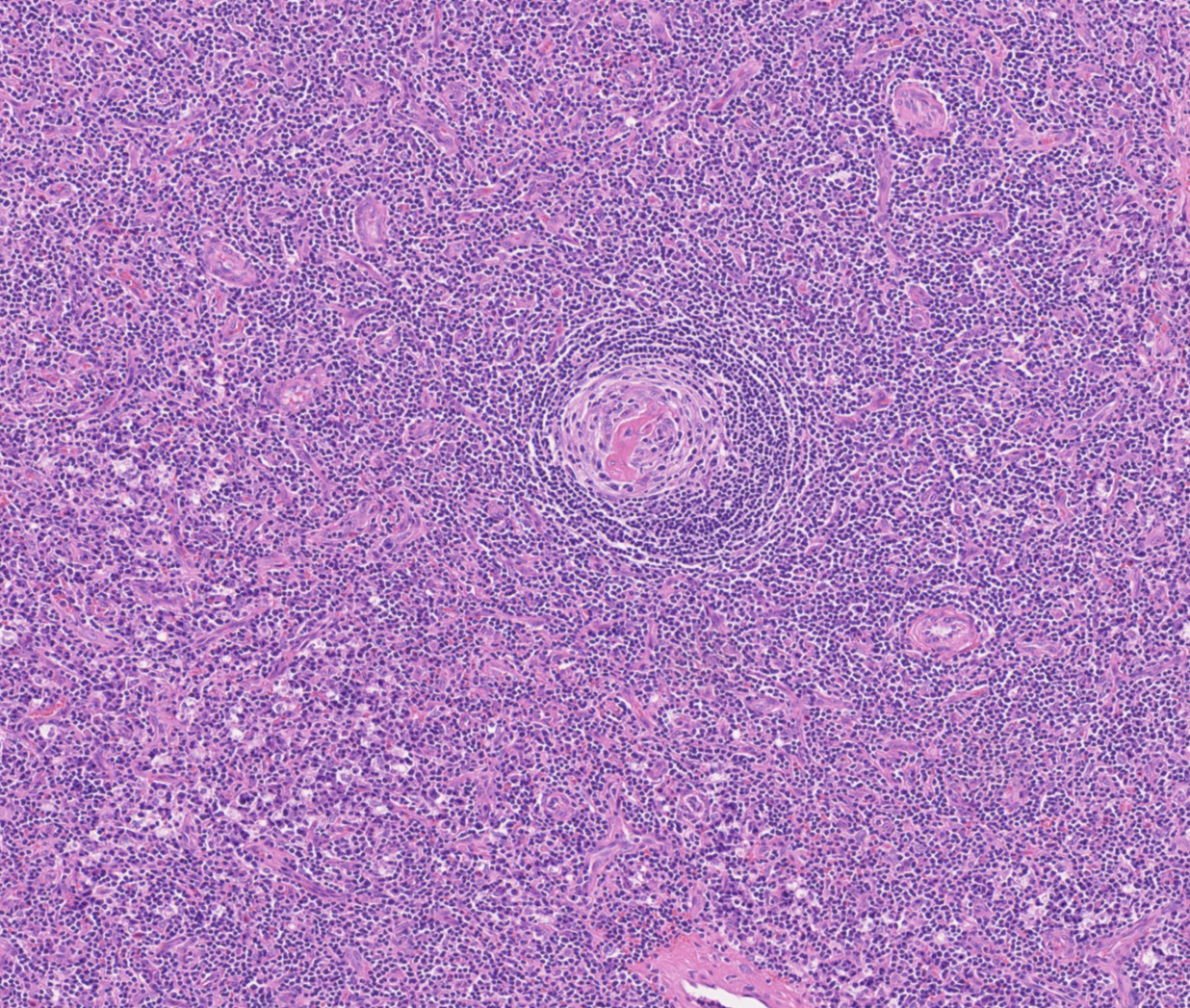
High power magnification revealed grade 2 plasmacytosis and grade 3 vascularity
Grading Insight
The biopsy was graded as Grade 2 plasmacytosis, Grade 3 follicular atresia, and Grade 2 vascularity, which correlated with severe systemic inflammation and guided treatment.
Treatment