CLINICAL VIGNETTES
CASE 2
A 34-year-old woman reports progressive fatigue, swelling in her legs, and abdominal fullness over six weeks. Examination reveals ascites and peripheral edema. Laboratory evaluation shows hypoalbuminemia, elevated IL-6 levels, and polyclonal hypergammaglobulinemia. Imaging reveals enlarged abdominal lymph nodes and effusions.
Misdiagnosis
The patient was initially diagnosed with systemic lupus erythematosus (SLE) and treated with corticosteroids for nearly a year. While symptoms partially improved, they recurred after steroid tapering.
Excisional Biopsy
An excisional lymph node biopsy revealed classic features of iMCD.
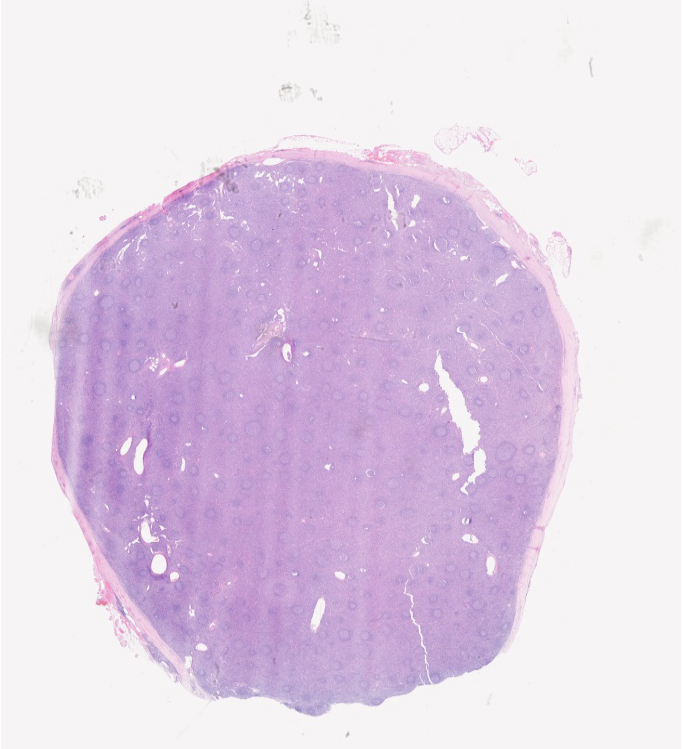
Learn about grading follicular atresia and view examples.
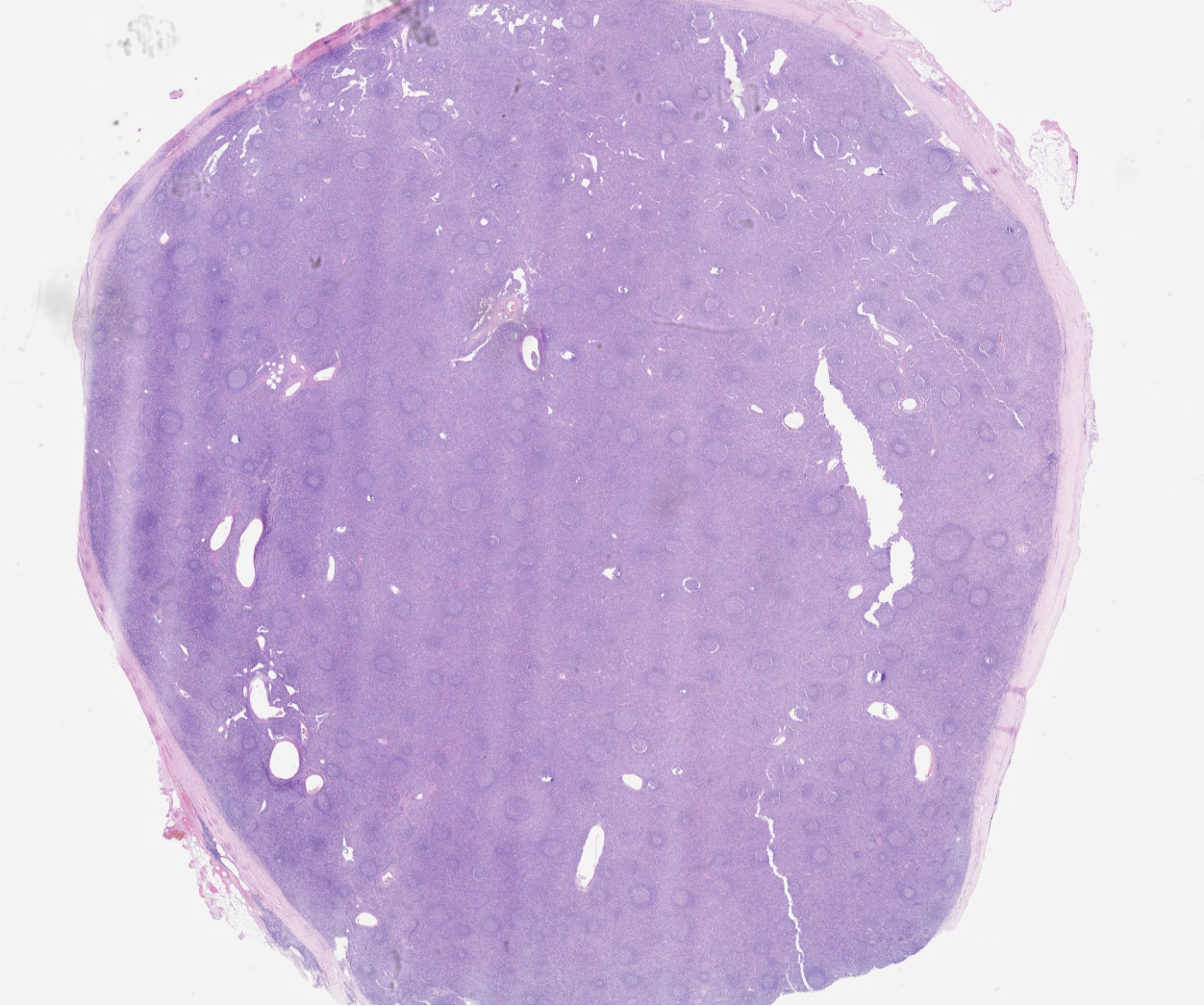
Follicular structures exhibited marked follicular atresia with depletion of germinal centers.
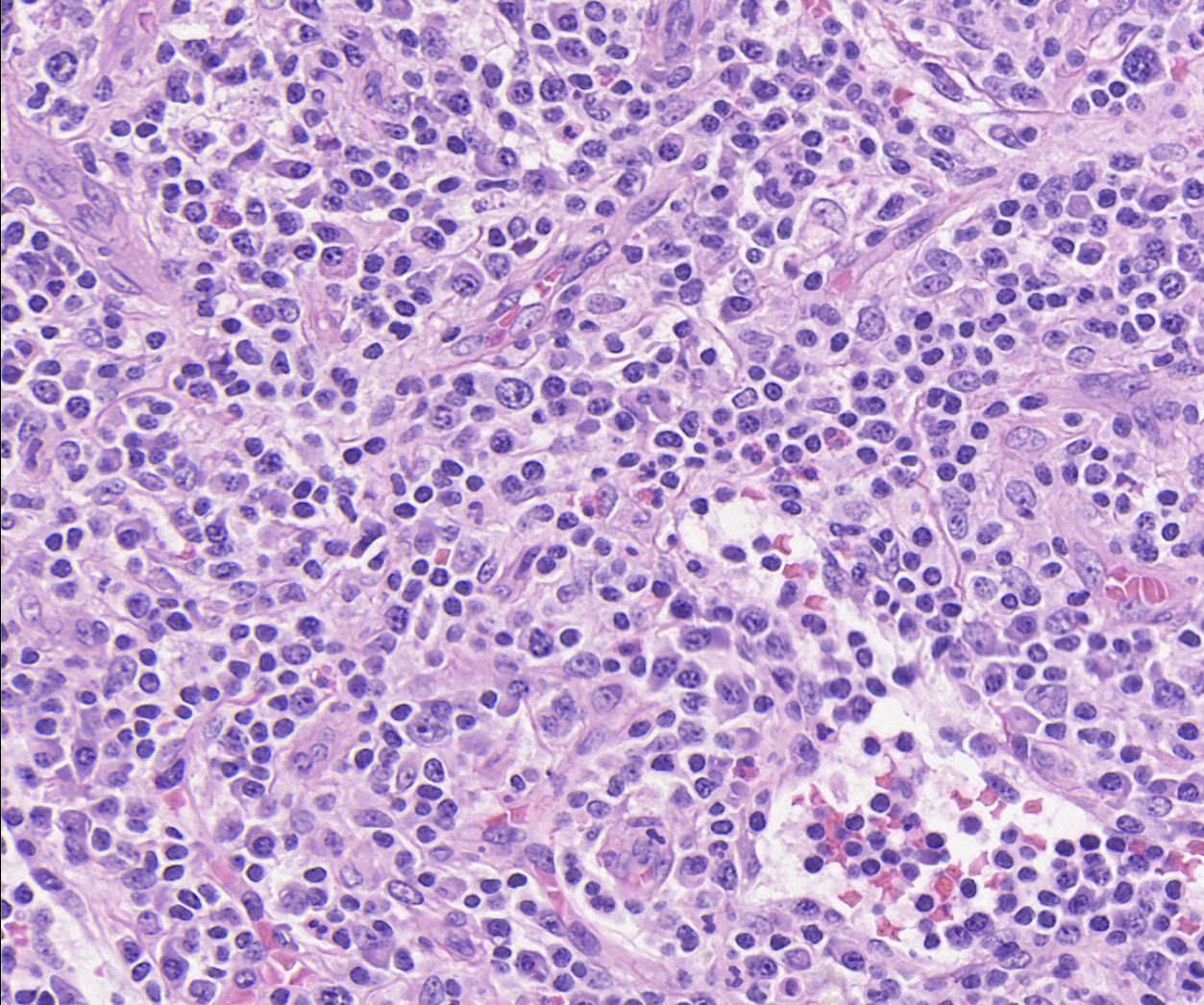
Plasmacytosis was prominent throughout the interfollicular regions.
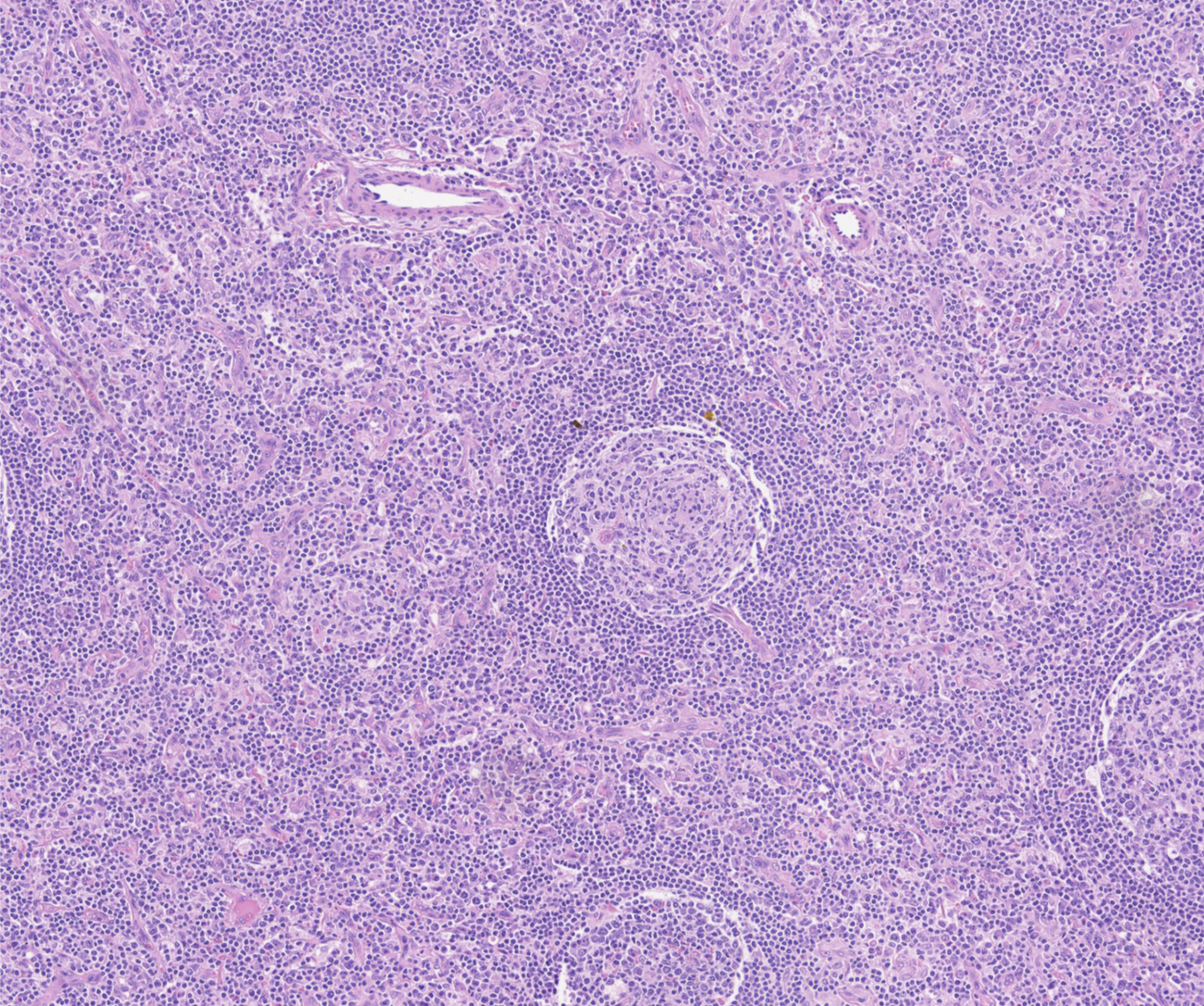
Higher-power analysis demonstrated grade 3 atrophic germinal centers
Grading Insight
The biopsy was graded as Grade 2 plasmacytosis, Grade 3 follicular atresia, and Grade 1 vascularity, consistent with Castleman disease.
Treatment